Tell me if this sounds familiar. The scale is dropping, clothes fit better, and colleagues have started to comment. And yet stepping into the gym, or walking up a flight of stairs, or lifting a suitcase into the overhead locker, the body feels less capable than it used to.
Feeling weak on Mounjaro is one of the most common things clients mention in our first conversation, and it’s almost always met with some version of the same apology. “I don’t know what’s wrong with me, I should be feeling great by now.” They shouldn’t be apologising. The weakness is usually signalling something specific, and it’s fixable, but only if the right thing gets addressed.
Nine times out of ten the answer is one of three things, often in combination: the caloric deficit is much larger than you realise, protein intake has fallen through the floor, or training is happening at a point in the injection cycle where recovery is already compromised. All three are addressable, and none of them are about willpower.
The 500-Calorie Ceiling
There’s a well-established threshold in the research on training during caloric restriction. A meta-analysis by Murphy and colleagues (2022) found that an energy deficit of roughly 500 calories per day prevented lean mass gain during resistance training, even when protein intake was adequate. Above that, the body stops putting on muscle. Push the deficit deeper and recovery starts to suffer too.
Most private-prescription GLP-1 users are well beyond 500 calories a day without realising it. The drug reduces total caloric intake by anywhere from 16 to 39% depending on dose, and some people drop below 800 calories a day during dose escalation. When a client tells me “I’m just eating less without trying,” the daily deficit often sits at 1,200 to 1,500 calories. That’s not a sustainable position for training hard.
So when sessions feel weak, the answer is usually to eat slightly more, not to train harder. More protein, and some carbohydrate around training days. On these drugs the real risk is accidentally eating half of what your body actually needs.
The Protein Shortfall
The second factor is almost always protein. For the reasons I’ve written about elsewhere, most GLP-1 users aren’t hitting the intake needed to support training recovery and lean mass preservation.
[INTERNAL LINK: how-to-keep-muscle-on-ozempic]
The target I use with clients is 1.6 grams of protein per kilogram of lean body mass per day. That’s the middle of the 1.2 to 2.0 g/kg range supported in the clinical nutrition literature on preserving lean mass in a deficit. For most adults it works out at 100 to 150g a day. For a deconditioned 95kg client starting treatment, usually around 120g.
When clients turn up saying training feels impossible, I ask them to track protein for three days. A typical result is 60 to 80g, roughly half of what’s needed. The training feels impossible because they’re under-fuelled for it, nothing more complicated than that.
Fixing it is mechanical. Front-load protein in the morning, aim for 40g at the first meal before the afternoon nausea dip. Keep easy-format protein available on injection day and the day after: Greek yoghurt, cottage cheese, shakes, eggs. Don’t skip meals, even when hunger is absent. The days where appetite disappears are the days protein needs most active defending.
Dose Escalation
The third factor is the dose phase itself. The first three to four months on Mounjaro, Ozempic or Wegovy are an active titration phase, where each new dose step brings a spike in GI side effects: nausea, reduced appetite, fatigue. The Wegovy SmPC puts the nausea rate on semaglutide 2.4mg at around 44%, peaking right after each dose increase.
That makes the first few months roughly the worst-case combination for training performance. Caloric intake is at its lowest, protein compliance is hardest, and GI side effects are at their peak. If you’re training hard through this phase and feeling weaker than usual, that’s a normal response.
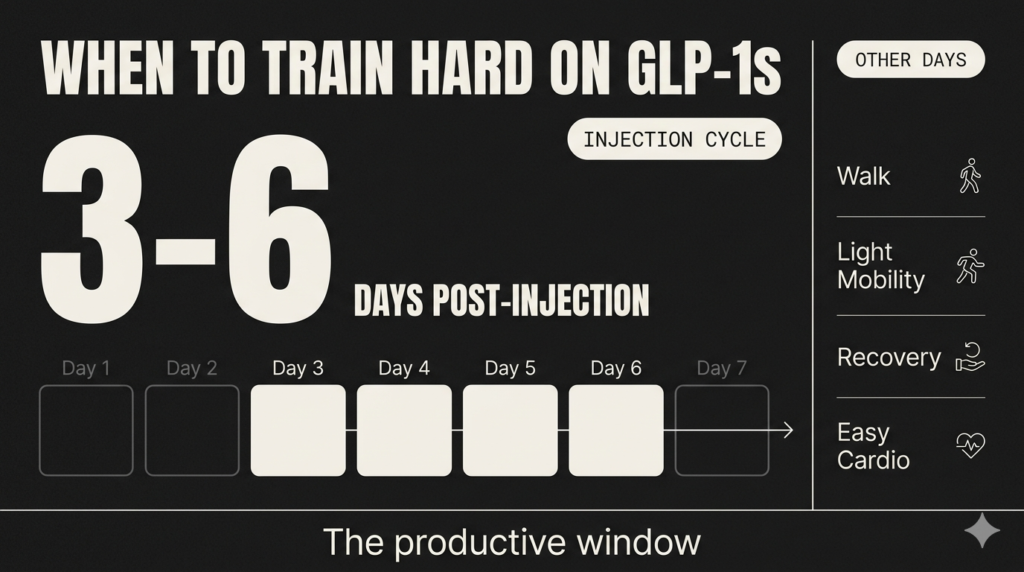
Two coaching changes help. Shift training to the productive window of the injection cycle, typically days 3 to 6 after injection. Reduce intensity to RPE 6 to 7 for the titration phase, while keeping frequency and volume intact. Strength will feel blunted for a couple of months and come back quickly once the dose settles at maintenance.
Strength Doesn’t Always Move With Bodyweight
Strength and lean mass don’t always move in the same direction during GLP-1 treatment. The same Murphy meta-analysis that found a 500-calorie deficit blocked lean mass growth also found that strength wasn’t impaired by the same deficit. The body defends performance before it defends tissue.
So “feeling weak” and “losing muscle” aren’t the same thing. It’s possible to be holding muscle and getting stronger on the drug while still feeling flat in individual sessions, because of low energy availability, GI distress, or poor sleep from a sudden dietary change. The fix for each of those is different.
If strength is genuinely going backwards on your main lifts over three or four weeks, there’s a problem worth investigating. A single session in the 24 hours after injection that feels awful is the injection cycle talking, not a trend.
The best metrics for cutting through the noise are strength tracking on your main compound movements, alongside bodyweight and waist. If the numbers on your working sets are holding steady or rising, the muscle is almost certainly fine, and the “weakness” is probably a recovery issue that’ll pass.
What to Do When You Feel Weak on Mounjaro
If this whole post describes you, a practical short-term plan looks like this:
- Protein audit: track for three days. If you’re below 1.6g per kg of lean body mass, front-load a 40g protein meal first thing and add a shake mid-afternoon. That alone is usually a 30 to 50g daily improvement.
- Deficit audit: if weekly weight loss is consistently over 1% of bodyweight, you’re in a very large deficit. Eat slightly more, especially around training days. Slower loss preserves more muscle.
- Training timing: shift the two main sessions of the week to days 3 to 6 after your injection. Rest or walk on the day of injection and the day after.
- Intensity taper during escalation: if you’re mid-dose-escalation, drop working sets to RPE 6 to 7 and hold frequency. Rebuild intensity at maintenance dose.
- Strength check: pick a couple of main lifts and track them weekly. Use those numbers as the truth-teller, not the scale.
Two weeks of the above, and most clients report sessions coming back. If they don’t, the next conversation worth having is with your prescriber, because persistent fatigue can sometimes indicate a dose that’s escalating too fast for your particular response.
If you want someone to build a training and nutrition programme that actually works around the drug you’re on instead of fighting it, I can help.